Bone Augmentation Using the BIONIKA Titanium Mesh
Background
Patient B. S., a 60-year-old woman, presented with a firm request to be relieved of the upper removable denture she had been wearing for more than ten years. Physical examination and 3D CBCT imaging both revealed marked bone involution. During consultations, the patient received detailed information about the available treatment options. Since she declined autogenous bone transplantation, the only viable path was to prepare the alveolar process for implant placement using the ridge-splitting technique, with bone substitute material applied as needed. In addition, sinus lift augmentation appeared unavoidable.
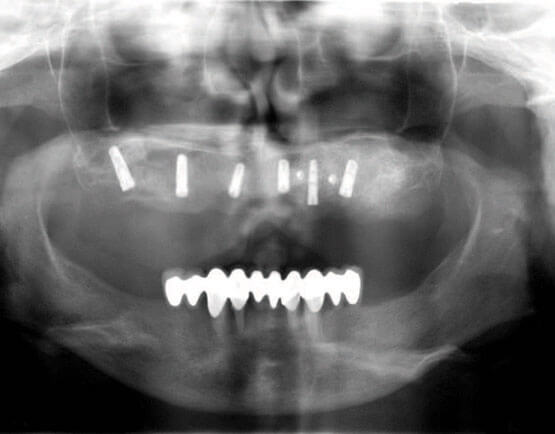
Postoperative panoramic radiograph
The Surgery
After appropriate preparation, bilateral crestal incisions were made. Due to the poor bone quantity and the blade-like thinning of the alveolar process, implant placement was performed using the ridge-splitting technique. Osteotomes were used to preserve as much native bone volume as possible. This approach allowed the placement of 3.8 mm diameter implants with correct positioning and good primary stability — except in the upper left canine region. Here the alveolar process was so severely thinned that even with slow, careful expansion, only a 3.3 mm diameter could be achieved.
During the final phase of careful implant insertion, the vestibular cortical plate fractured, exposing virtually the entire implant surface along its full length. This circumstance threatened to derail the planned treatment entirely — the promise made to the patient seemed about to dissolve, and a significantly longer, multi-stage treatment course appeared to be the only alternative. At that moment, a solution presented itself. A few months earlier, we had established contact with BIONIKA and had purchased their 0.2 mm titanium mesh along with the corresponding fixation screws. Fortunately, both were available in sterile, ready-to-use condition. The mesh was easily customized with scissors to match the anatomical situation and adapted to the surface of the alveolar process. Bone chips collected during the placement of the other implants were mixed with bone substitute material (OSSEO+B-3M COMPANY). The resulting mixture was applied in a 2–3 mm layer over the vestibular surface of the alveolar process, fully covering the damaged bone surface with slight over-contouring. The adapted titanium mesh was placed over this graft and secured with two screws, after which the mucoperiosteum was closed in a single layer with continuous atraumatic mattress sutures.
Following an uneventful postoperative course and primary wound healing, the patient resumed wearing her adjusted upper denture,
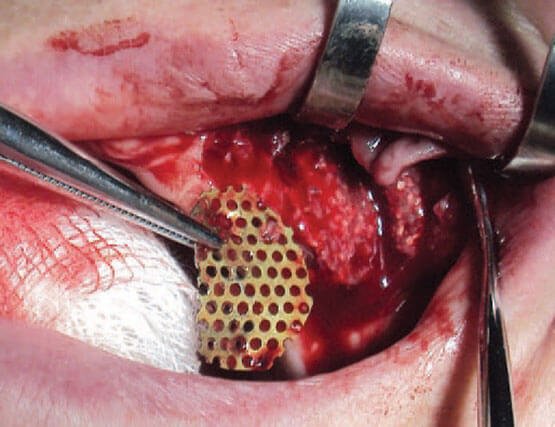
The adapted mesh at the time of removal
and two months later the titanium mesh was removed. The bone substitute had integrated successfully and the contour of the alveolar process had normalized. Two months after that, implant uncovering was performed according to best practice, followed by prosthetic rehabilitation with a fixed bridge.

Completed abutments in situ

The final result
Conclusions
The method described above appears well suited for cases in which fixation of a bone graft or bone substitute material requiring adequate mechanical protection is the primary objective. The titanium mesh eliminates micromovement and ensures contour stability.
Article information
- Author | Dr. Joós Gyula
- Date | 2014. 01.01
- URL | www.bionika.hu